
-
Home
-
Product

-
IMMUNOHISTOCHEMISTRY
-
INSTRUMENT
-
MOLECULAR
-
HISTOLOGY
-
CYTOLOGY
-
DIGITAL PATHOLOGY
-
-
Solution
-
Support
-
About
-
Contact

Breast Cancer Pathology
Pathology is the branch of medicine that looks at how disease affects the body’s cells and tissues. Tissue removed from the body (for example, during a biopsy or surgery) is looked at under a microscope, and may have tests performed on it. The results are given in a pathology report that explains the type of breast cancer and its features. Pathology results can also come from tests called genomic assays but these are not suitable for everyone. Breast cancer pathology results are important in helping your specialist team decide which treatments might work best for you, and also help to estimate the chance of the breast cancer coming back (recurrence).
IHC is an increasingly common method used in the diagnosis of breast cancer and research into breast cancer pathology. There is an increasing number of antibodies available for the detection of breast cancer-specific markers. These markers are used to determine different breast cancer types, e.g. in situ or invasive carcinoma, distinguishing normal breast cell types e.g. luminal, basal and myoepithelial, and also proliferation and disease progression (Zaha et al., 2014).
The presence of estrogen receptors (ERs), as detected by immunohistochemistry (IHC), is a weak prognostic marker of clinical outcome in breast cancer, but a strong predictive marker for response.
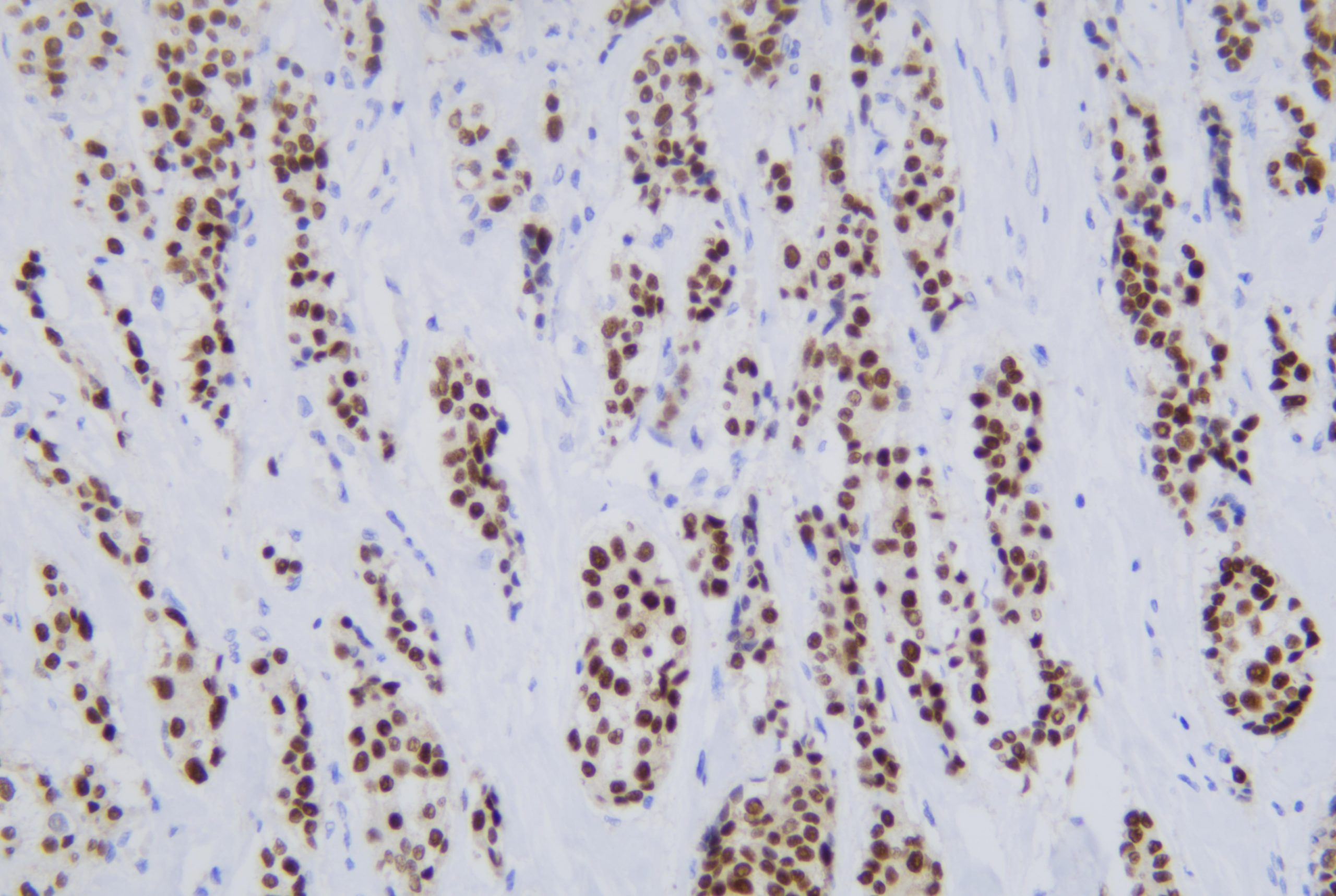
Celnovte ER-breast cancer-200×
Recommended antibody:https://www.celnovte.com/estrogen-receptor-er/
The progesterone receptor (PR) is another biomarker important for the initial diagnosis and evaluation of breast cancer (Hicks et al., 2017).
Celnovte PR-breast cancer-200×
Recommended antibody:https://www.celnovte.com/progesterone-receptor/
Ki67 is an important protein involved in cell division and is commonly used as a marker of cellular proliferation. It is also used in breast cancer diagnosis to determine the level of cell proliferation which can be a prognostic marker and a good indication of well certain breast cancers will respond to endocrine therapy (Niazi et al., 2018). Ki67 is a protein found in cells. The higher the levels, the faster the cells are dividing and growing. Ki67 is not usually included in pathology results. If it is, the report will say what percentage of the breast cancer cells test positive for Ki67. Less than 10% is considered low, 10–20% is medium and more than 20% is high. The higher the score, the faster the cells are dividing and growing.
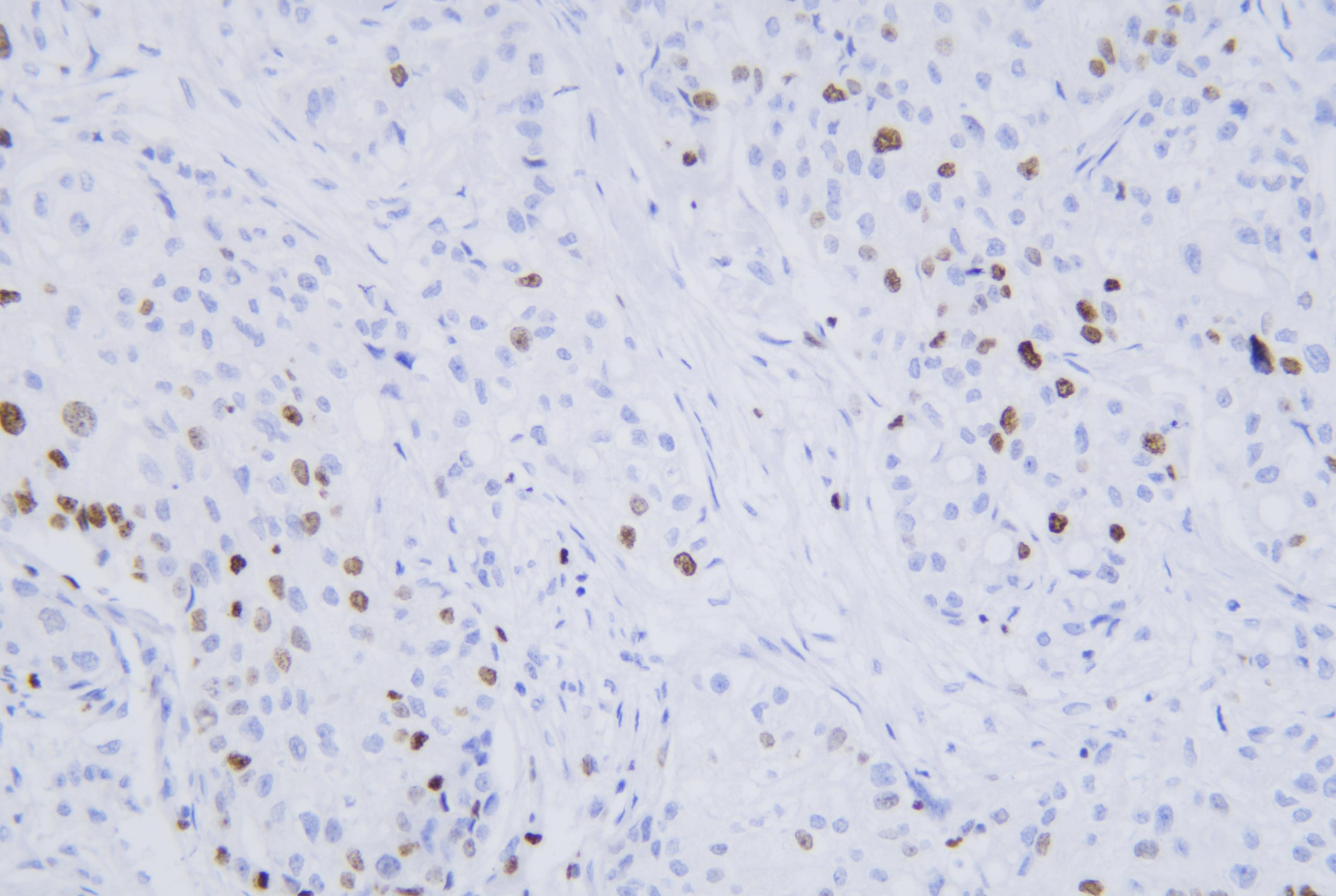
Celnovte Ki-67-breast cancer-200×
Recommended antibody:https://www.celnovte.com/ki-67-antigen/
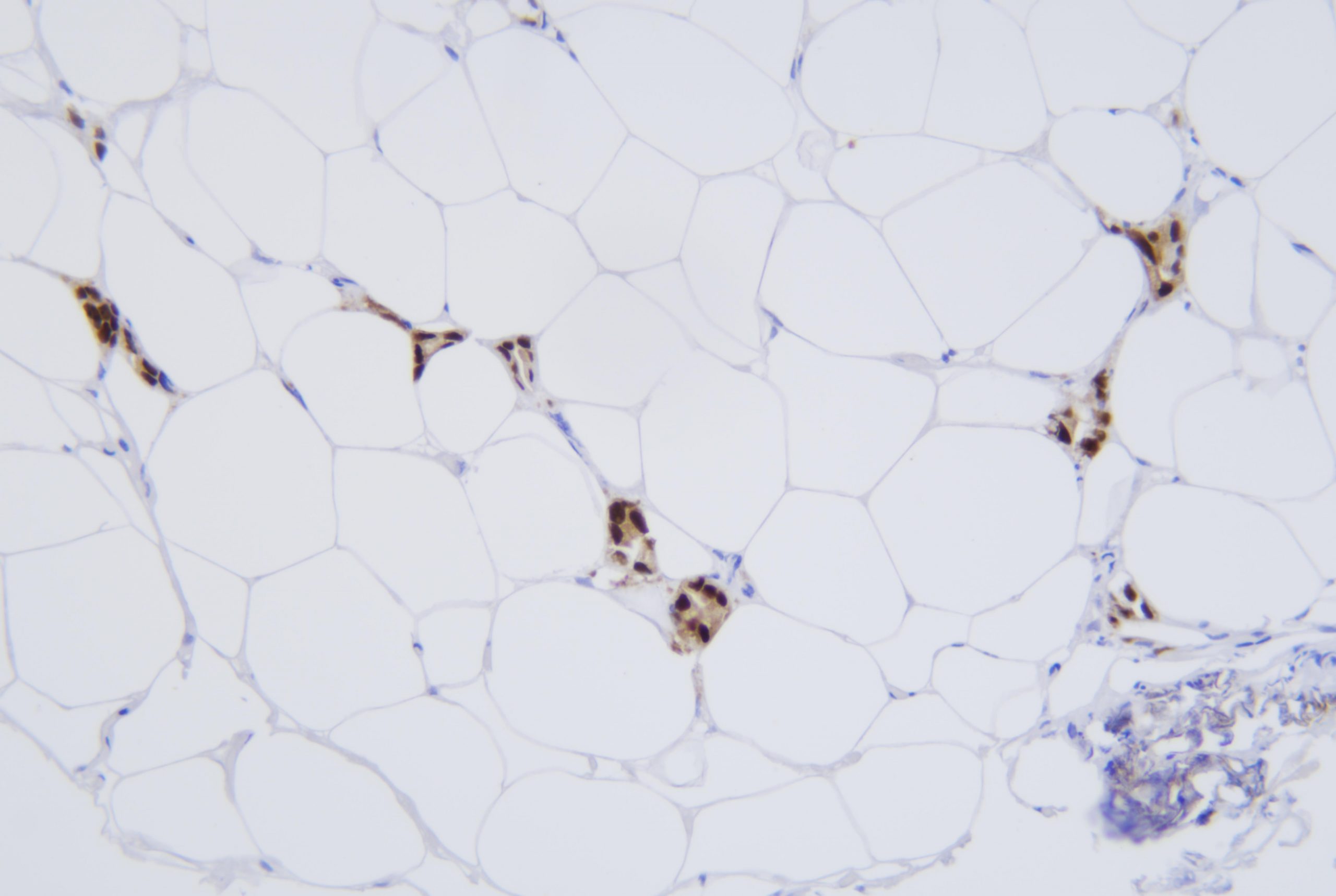
Around 15–20% of breast cancers have a higher than normal level of a protein called HER2 on their surface, which stimulates them to grow. These cancers are called HER2 positive or HER2+. Generally they are more likely to grow and spread faster than most types of HER2 negative breast cancers. All invasive breast cancers are tested for HER2 levels. The results can sometimes take longer than the rest of the pathology results but are usually available between one and three weeks after your biopsy or surgery.
There are various tests to measure HER2 levels. The four most commonly used tests are IHC (immunohistochemistry), FISH (fluorescent in situ hybridisation), CISH (chromogenic in situ hybridisation) and DDISH (dual-colour dual-hapten brightfield in situ hybridisation).
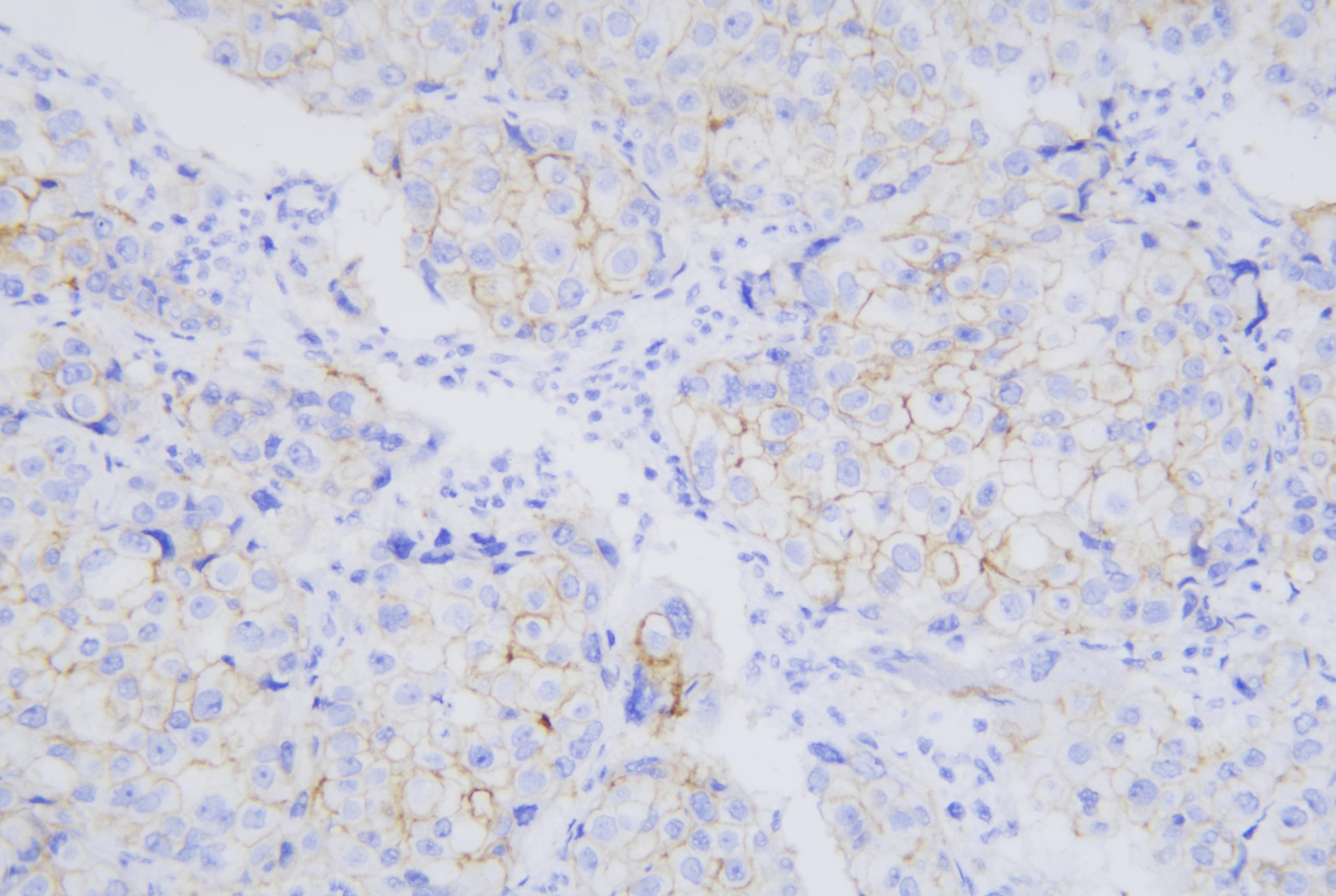
Celnovte HER2-breast cancer-200× (IHC)
Recommended antibody:https://www.celnovte.com/c-erb-2-oncoprotinher-2/
IHC is usually done first. It involves a special staining process performed on a sample of breast cancer tissue. It’s reported as a score ranging from 0–3+. A score of 0 or 1+ means the breast cancer is HER2 negative. A score of 2+ is borderline and a score of 3+ means the breast cancer is HER2 positive. Breast cancers with a borderline result (2+) should be retested with FISH, CISH or DDISH to find out if they are HER2 positive. These are more specialised tests and are usually reported in pathology results as positive or negative.
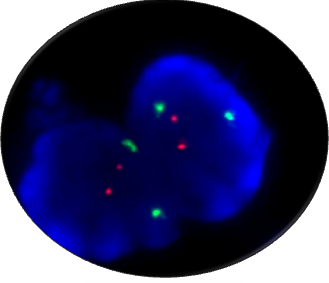
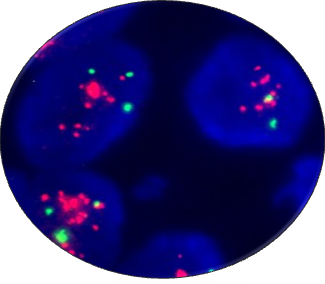
FISH HER2 Normal FISH HER2 Gene Amplification
Recommended FISH probe:https://www.celnovte.com/her2-gene-amplification-detection-kit/
More details please contact us on email info@celnovte-bio-tech.com
References
Hicks, D., Dell’Orto, P., Falzon, M., Hoff, K. D., Levy, Y. Y., McMahon, L., … Viale, G. (2017). Immunohistochemical performance of estrogen and progesterone receptor antibodies on the dako omnis staining platform: Evaluation in multicenter studies. Applied Immunohistochemistry and Molecular Morphology, 25(5), 313–319.
Niazi, M. K. K., Senaras, C., Pennell, M., Arole, V., Tozbikian, G., & Gurcan, M. N. (2018). Relationship between the Ki67 index and its area based approximation in breast cancer. BMC Cancer, 18(1), 1–9.
Zaha, D. C. (2014). Significance of immunohistochemistry in breast cancer. World Journal of Clinical Oncology, 5(3), 382–392.
https://breastcancernow.org/sites/default/files/publications/pdf/bcc161_understanding_your_pathology_results_web.pdf
https://www.nature.com/articles/modpathol200834