
-
-
SHOP




PolyStacker™ Technology Offers Unique Solutions in Frozen Section IHC
 2024-04-30
2024-04-30
By celnovte
Table of Contents
- Background
- Case Studies
- Product Catalog
Background
For cancer patients, the world of treatments is rapidly changing and growing, offering cutting-edge technology, and promising new methods of fighting the disease. But as all journeys must begin with a first step, so does the path to recovery in cancer treatment, and this first step traditionally involves hematoxylin and eosin (H&E) staining. Intraoperative frozen-section consultation is one such avenue of H&E frequently used, where slides are prepared from frozen tissue mass. H&E staining is a rapid enough process to generate results usually within 30-60 minutes.
This method has issues however, particularly with the freezing process damaging tissue morphology, making the results difficult to interpret. Unfortunately, oftentimes these difficulties lead to misdiagnosis, necessitating further testing or even repeating surgery for the patient – a process that is taxing in time, money, and mental stress for all involved.
Immunohistochemistry (IHC) staining offers a solution to this by increasing operator confidence compared to H&E staining, since IHC staining shows biomarker expression in addition to the general morphology of the tissue. The drawback to this historically, however, is that the process can be very time-consuming and can take hours to complete. With that turnaround rate, IHC is not used during the intraoperative phase despite its advantages, restricted to post-operational diagnostics, where it can take 1-2 days to process and interpret. During this time, surgeons may need to decide on how to proceed without having complete certainty in what they’re dealing with.
But what if speed was no longer a factor? Celnovte Biotechnology’s PolyStackerTM detection technology guarantees results within the acceptable timeframe with a turnaround time as short as 10-15 minutes to assist in diagnosing cancer – all intraoperatively. This rapid IHC protocol is used in parallel with H&E staining to give a full picture of the nature of the tissues sample, assisting surgeons in making decisions for next steps.
The technology promises rapid detection of tumor markers, reduced false negative rates, increased accuracy in diagnosing challenging cases (metastatic microlesions, infiltrative microlesions) and comparable match rates to post-operative traditional FFPE IHC results. With this, surgical decisions can be made with increased confidence and less stress for patients and surgeons alike, allowing for more informed decision making when choosing the next steps in treatment and can save precious time in the fight against cancer.
Case Studies
The efficacy of Celnovte Biotechnology’s frozen section rapid IHC technology can be observed in the following case study. In this example, doctors in China cite an example of lung cancer where rapid IHC was used. The patient, a 67-year-old female, was admitted to the hospital and underwent surgical treatment due to nodules seen in a CT scan that were not responsive to anti-inflammatory treatment.
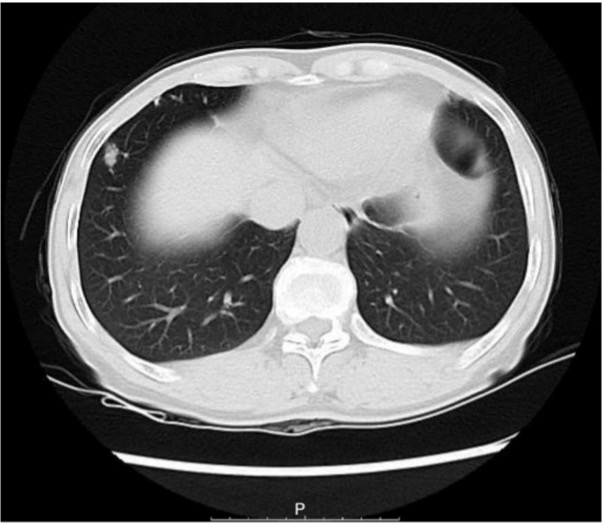
Figure 1 – CT scan of patient in case study 1, the bilateral thorax was symmetrical, and no obvious abnormalities were found. The trachea is centered, and the tracheobronchial tree is unobstructed. A solid nodule (thin layer lm373) was found in the lower lobe of the right lung, with a long diameter of approximately 11.3 mm. There are a few micronodules in both lungs. The structure of the bilateral lung hilum was clear, and there were no obvious abnormalities in shape, size, and position. There was no abnormal enlargement of lymph nodes in each group of mediastina.
Frozen section diagnosis was used to determine the nature of the nodules to determine malignancy of the observed growths. The patient underwent partial lung tissue resection of the right lower lobe which was sent for freezing and used in both H&E as well as rapid IHC tissue testing.
For H&E, many lymphocyte cells were seen, however no obvious malignant lesions were found.
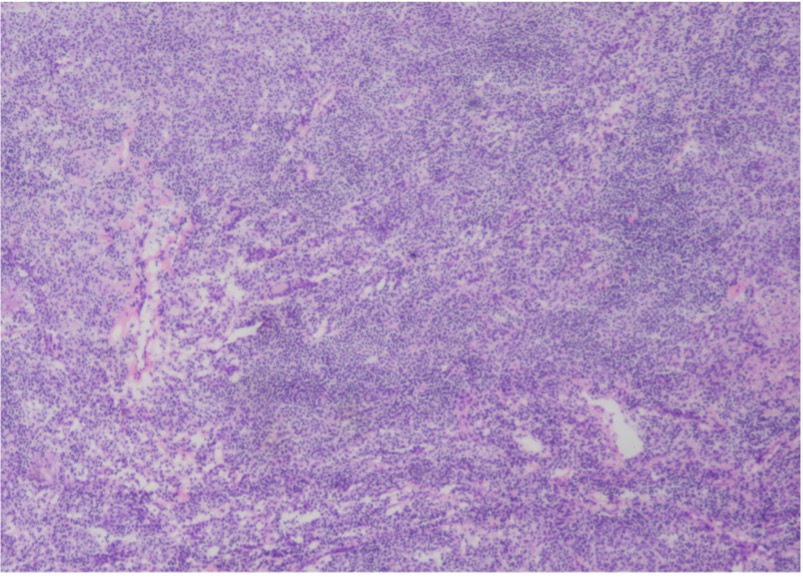
Figure 2 – H&E staining of tissue section from lower right lung, 120x40x15mm in size. Lymphoid tissue proliferation was seen in the sections, and no obvious malignant lesions were found under routine H&E staining.
Due to the application of rapid IHC for the frozen section, it can be observed that small focal clusters of epithelial cells were seen in the sections via CK staining, which was considered an epithelial malignant tumor.
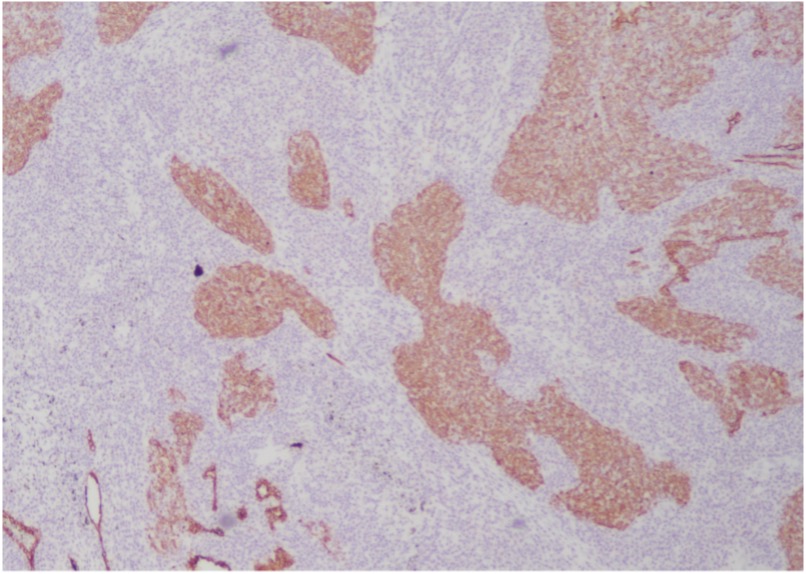
Figure 3 –Celnovte Biotechnology frozen section rapid IHC staining of tissue section from lower right lung, 120x40x15mm in size. After CK staining, small focal clusters of epithelial cells were seen in the sections, which was considered an epithelial malignant tumor.
In conjunction with the H&E staining results, surgeons were able to intraoperatively move forward with the working assumption that the tissues were positive for lymphoepithelial carcinoma, an assumption they would’ve been unable to make in the operating room if they had only used H&E staining. Further FFPE IHC testing with CK, P40 and in situ hybridization EBER and a noted absence of nasopharyngeal tumors confirmed the assumption and diagnosed the patient with lymphoepithelial carcinoma.
In this case, Celnovte Biotechnology’s frozen section rapid IHC was used to show the presence of difficult to see lymphoepithelial carcinoma cells. Due to the large volume of lymphocytes in the selection, it would be especially difficult to see these squamous/undifferentiated cells as they can be overshadowed with so few and small cell clusters. Because of the use of rapid IHC, the diagnosis was correctly made where it would otherwise be easy to misdiagnose these tumor cells despite them being in the early stages of growth where lesions are less obvious.
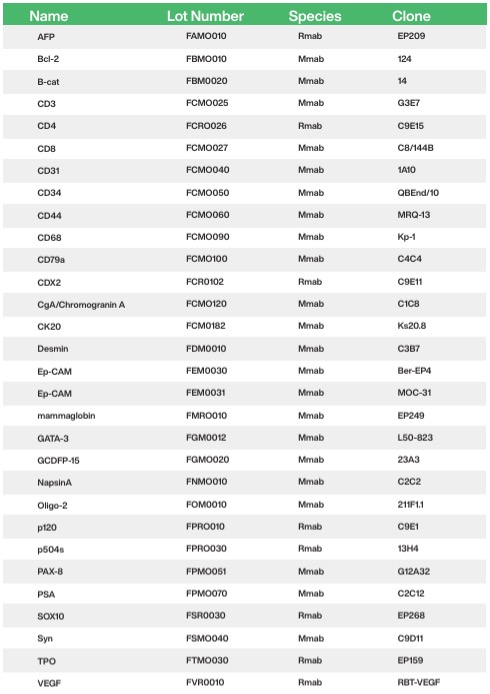
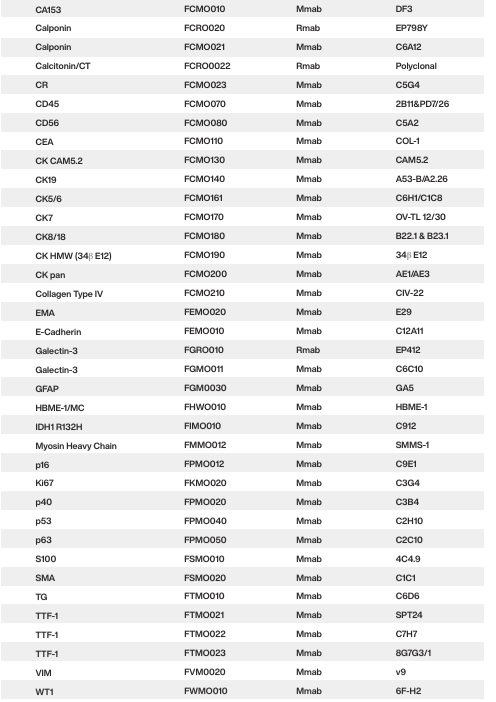
Product Catalog
📣 Contact us now
Celnovte is a rapidly expanding global company, and we invite you to join us in growing our businesses together. ☺️ Contact us now


,MMab")

