
-
-
SHOP

Gastrointestinal Tumor diagnosis & IHC markers
![]() 2023-10-31
2023-10-31
By celnovte
1. HER2
HER2 is amplified and/or overexpressed in 9% to 27% of adenocarcinomas of the stomach and gastroesophageal junction. It occurs more frequently in intestinal-type tumors than in diffuse-form tumors and is more common in well to moderately differentiated tumors than in poorly differentiated tumors. Detection of HER2 in gastric and gastroesophageal junction adenocarcinomas by immunohistochemistry of biopsy or resection specimens has become routine practice among pathologists.
Current guidelines recommend the use of trastuzumab to treat tumors with a HER2 score of 3+ or a score of 2+ with evidence of HER2 amplification by in situ hybridization (ISH). Trastuzumab is not recommended for tumors with a score of 0 or 1+. Therefore, fluorescence ISH assay (FISH) or other ISH methods should be performed by immunohistochemistry on 2+ tumors, although immunohistochemistry and FISH can be performed routinely in all cases at some institutions. When performing ISH, it is important to assess the signal in areas showing HER2 immunoreactivity.
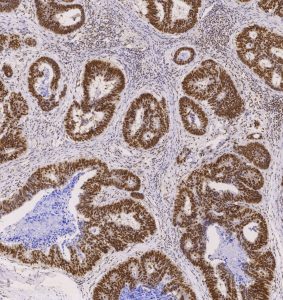
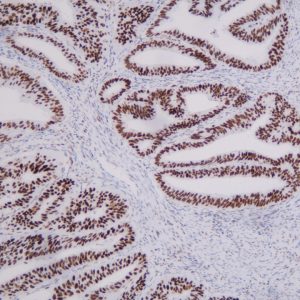
2. MMR
Mismatch Repair (MMR) is a repair method that restores the nucleotide sequence to normal in DNA molecules containing mismatched bases.The MMR system can involve several mismatch repair proteins when participating in DNA repair, among which, MLH1, MSH2, MSH6, and PMS2 are the dominant proteins in MMR.
Immunohistochemistry (IHC method) is the recommended method for MMR detection in relevant guidelines.
Positive expression of all four MMR proteins in a tumor sample is considered as complete mismatch repair (pMMR); absence of any of the MMR proteins is considered as defective mismatch repair (dMMR).The results of the IHC assay are indicative of the subsequent mutation detection of the MMR genes.
MMR testing is important for the prediction, prognosis, and treatment of various tumors such as colorectal, gastric, and endometrial cancers, as well as the diagnosis of Lynch syndrome.
3. CK7 and CK20
CK7 and CK20 belong to the Cytokeratin (CK) family, which is mainly used in the diagnosis and differentiation of tumors of epithelial tissue and epithelial origin. CK7 is considered to be a specific marker for adenocarcinoma and metastatic epithelial cell carcinoma, and can be used in the differential diagnosis of renal cell carcinoma, smoky cell carcinoma, and eosinophilic cell carcinoma.The expression of CK20 is consistent between primary cancer foci and lymph node metastasis, which is important for the determination of the origin of small-cell tumors.The combination of CK20, CK7, and Villin has been used as an indicator for the site of origin of the carcinoma.CK20 and CK7 are used as a marker of the primary site of the cancer.CK20 is also used as an indicator of the primary site of the cancer.
Differential expression patterns of CK7 and CK20 are commonly used in the examination of adenocarcinomas of unknown primary. In colorectal cancer, CK20 positivity is usually diffuse, whereas CK7 immunoreactivity, if present, is usually focal or patchy.CK7 expression in colorectal cancer may also be lower than in non-colorectal adenocarcinomas that normally express CK7. Most gastroesophageal adenocarcinomas and pancreaticobiliary adenocarcinomas are CK7+/CK20-, but a few cases are CK7+/CK20+ or even CK7-/CK20+. Anal adenocarcinoma may be histologically confused with rectal adenocarcinoma, which is usually also CK7+/CK20-. The tumor is also CDX2-negative and may show absent expression of p63 and CK5/6 proteins.
4. Desmin
Desmin is a 53 kDa intermediate filament protein found mainly in cardiac, smooth muscle and rhabdomyocytes. Benign and malignant tumors of the above cellular origin desmin show a positive response. It is mainly used in the diagnosis and differential diagnosis of uterine, skin and gastrointestinal smooth muscle tumors, rhabdomyosarcoma and myoepithelial tumors.
Reports of smooth muscle sarcomas of the gastrointestinal tract show desmin positivity in 33% to 100% of cases; as with SMA, the degree of positivity correlates with the grading of the tumor, with higher graded smooth muscle sarcomas less likely to be positive. In addition, there are few studies addressing the immunophenotype of smooth muscle sarcomas, which explains the wide variation in desmin expression. It is also noteworthy that some cases considered desmin-positive show focal staining in only 5% to 10% of tumor cells; this may be problematic for needle biopsies or small samples, which may not be representative of the entire lesion.
Although Desmin is a sensitive marker of myogenic differentiation, it may also show positive expression in tumors with myofibroblast differentiation, such as fibromatous lesions. Desmin positivity has been reported in up to 5% of fibroma-like fibrous tumors. In addition, desmin is positive in approximately 5% to 10% of GISTs. However, positivity is more common in tumors with epithelioid cells (10%) compared to tumors with spindle cells (2.5%). Notably, other markers of smooth muscle differentiation, such as h-caldesmon, are usually positive in GIST.
, MMab")